Plain English Summary (short)
Contents
Plain English Summary (short)#
Stroke is a common cause of adult disability. Expert opinion is that about one in five patients should receive clot-busting drugs to break up the blood clot that is causing their stroke. At the moment only about one in nine patients actually receive this treatment in the UK. There is a lot of variation between hospitals, which means that the same patient might receive different treatment in different hospitals.
Figure 2 shows a summary of the percieved problem.
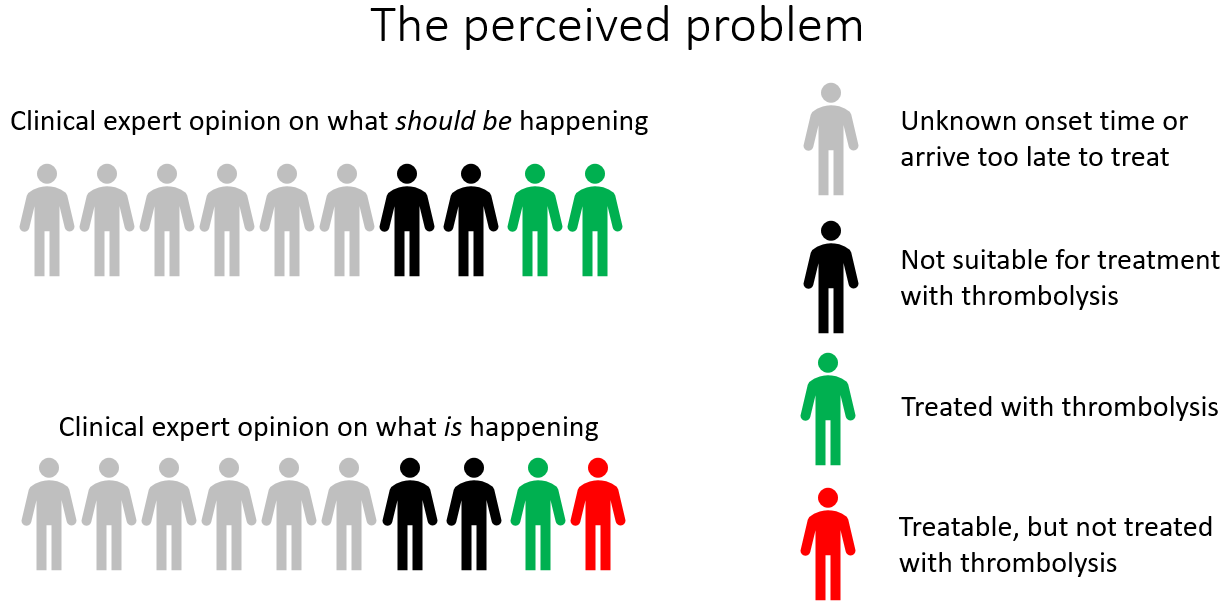
Fig. 2 A summary of the peceived problem. Clinical expert opinion is that two in every ten emergency stroke patients could be treated with thrombolysis, but the reality is that only about one in ten are treated with thrombolysis.#
Clot-busting drugs are not suitable for everyone. Doctors must feel confident in their use, and lack of confidence may explain some of the variation in use. Hospitals must also be well set up to be able to investigate and treat stroke patients quickly, like getting them to a head scanner quickly (an essential step before treating).
In our work we have developed the methods for understanding what are the main causes of variation between hospitals: How much difference is due to processes (like how quickly a patient is scanned), how much is due to differences in patient populations, and how much difference is due to different decision-making by doctors.
For each hospital we can say what would have the most effect – is it the decision-making (lack of confidence), is it that the processes, like scanning, need to be sped up, or is it that the hospital needs to find a way of better finding out when a person has had a stroke (if that is unknown then it is not possible to give clot-busting drugs)?
By using these methods we predict that the number of people across England and Wales for whom clot-busting drugs would prevent disability after stroke could be nearly doubled.
Along the way we interviewed doctors on their thoughts of what we were doing. Though they were interested in our work, some needed to know more about how our methods work before they felt they could trust them.
Summary of findings#
Figure 3 shows a summary of the percieved problem and what we found by using modelling the pathway and the clinical decision-making.
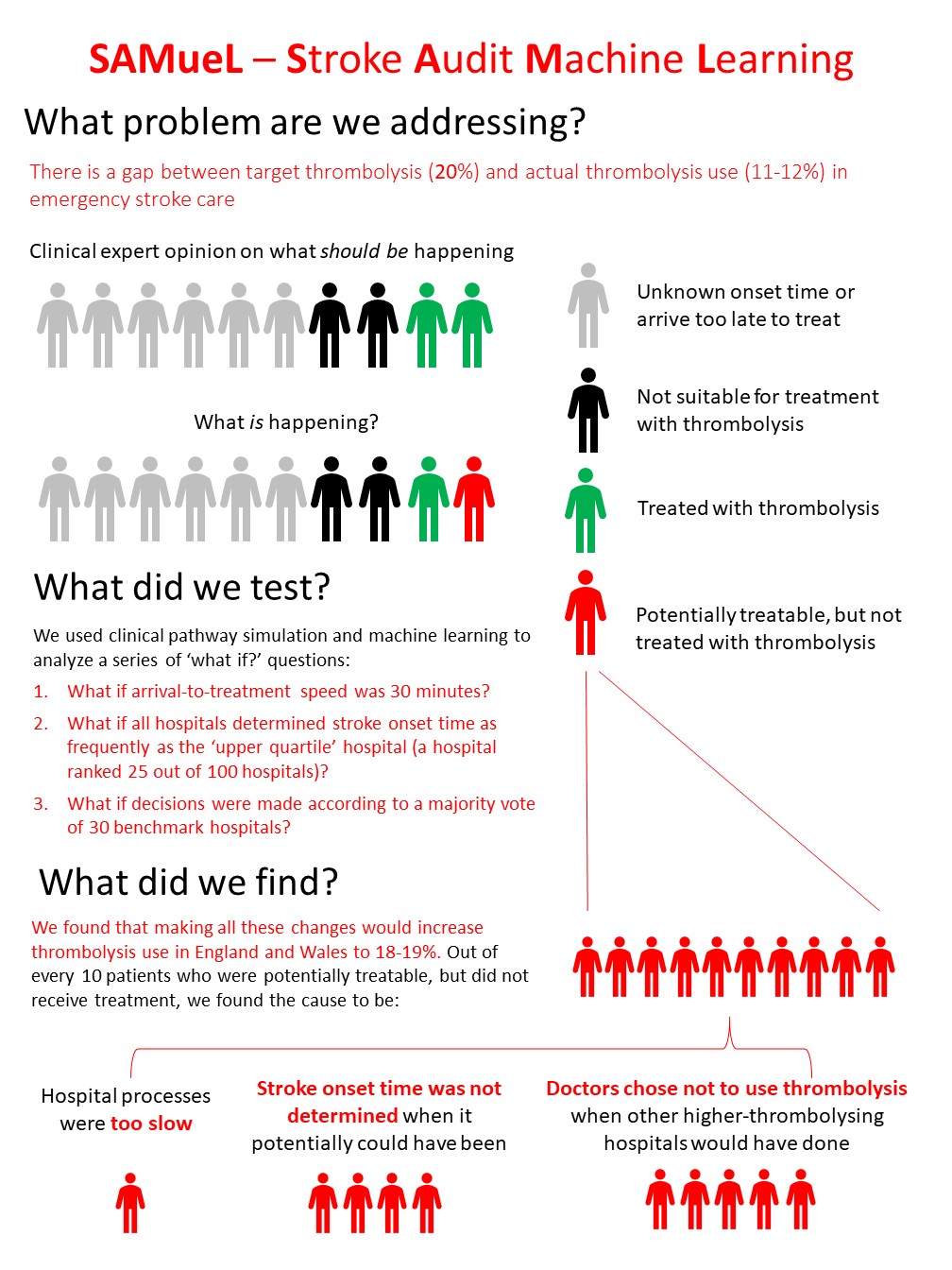
Fig. 3 A summary of the perceived problem and our findings. Clinical expert opinion is that two in every ten emergency stroke patients could be treated with thrombolysis, but the reality is that only about one in ten are treated with thrombolysis. This leaves about one in ten patients who could be treated, but are not. For patients who might be treated but were not, we found the main cause is likely to be variation in clinical decision-making between hospitals. After decision-making the change that would make the most difference was increasing the proportion of patients with known stroke onset time, to be at least the current national upper quartile. Finally speed increases would improve the use of thrombolysis a little (but would also benefit everyone who does receive thrombolysis, as the faster the treatment the better the likely outcome).#